Abbracs
- TABLE OF CONTENTS
- 1 INTRODUCTION
- 2 SCOPE
- 3 GUIDELINES ON ABBREVIATION AND ACRONYM USAGE
- 4 ACCESSIBILITY
- 5 TAXONOMY OF ABBREVIATION AND ACRONYM USAGE
- 6 RESEARCH AND PROTOTYPING
- 7 REFERENCES
- APPENDIX A JOINT COMMISSION ON ACCREDITATION
- APPENDIX B INSTITUTE OF SAFE MEDICAL PRACTICE (US)
- APPENDIX C POTENTIALLY DANGEROUS AMBIGUOUS ABBREVIATIONS AND ACRONYMS
- REVISION AND SIGNOFF SHEET
- Change Record
- Reviewers
- Distribution
- Document Properties
 Prepared for
NHS Connecting for Health
Version 1.0.0.0 Baseline
Prepared by
Mark A. Wilson-Thomas
Program Manager
cuistakeholder.mailbox@hscic.gov.uk
This document was prepared for NHS Connecting for Health which ceased to exist on 31 March
2013. It may contain references to organisations, projects and other initiatives which also no
longer exist. If you have any questions relating to any such references, or to any other aspect of
the content, please contact cuistakeholder.mailbox@hscic.gov.uk
Prepared for
NHS Connecting for Health
Version 1.0.0.0 Baseline
Prepared by
Mark A. Wilson-Thomas
Program Manager
cuistakeholder.mailbox@hscic.gov.uk
This document was prepared for NHS Connecting for Health which ceased to exist on 31 March
2013. It may contain references to organisations, projects and other initiatives which also no
longer exist. If you have any questions relating to any such references, or to any other aspect of
the content, please contact cuistakeholder.mailbox@hscic.gov.uk
1 INTRODUCTION
- 1 INTRODUCTION
- 2 SCOPE
- 3 GUIDELINES ON ABBREVIATION AND ACRONYM USAGE
- 4 ACCESSIBILITY
- 5 TAXONOMY OF ABBREVIATION AND ACRONYM USAGE
- 6 RESEARCH AND PROTOTYPING
- 7 REFERENCES
- APPENDIX A JOINT COMMISSION ON ACCREDITATION
- APPENDIX B INSTITUTE OF SAFE MEDICAL PRACTICE (US)
- APPENDIX C POTENTIALLY DANGEROUS AMBIGUOUS ABBREVIATIONS AND ACRONYMS
- REVISION AND SIGNOFF SHEET
Source PDF: abbracs.pdf
This document presents design principles and guidance that describe how NHS clinical applications should handle abbreviations and acronyms in input and display fields. This design information uses principles from reviews of relevant literature, best practices and published glossaries.
This document also suggests areas for future research. This research and prototyping would allow further validation of some of the guidance.
1.1 Summary of Recommendations
NHS clinical applications should:
- Require the user to resolve known dangerous abbreviations and acronyms, especially when
a user enters information as free text.
- Avoid abbreviations or provide readily accessible explanations when displaying labels
(screen text).
- Present abbreviation punctuation and capitalisation consistently.
1.2 Recommendations Requiring Future Research
Research should be performed to validate these recommendations.
When allowing free-text input which includes abbreviations, applications can:
- Use an interface to alert the user entering the information, who can then resolve any
unexpanded abbreviations and acronyms
- Provide warnings for any remaining unexpanded abbreviations and acronyms when users
view this information.
Page 2
Copyright ©2013 Health and Social Care Information Centre
HSCIC Controlled Document
2 SCOPE
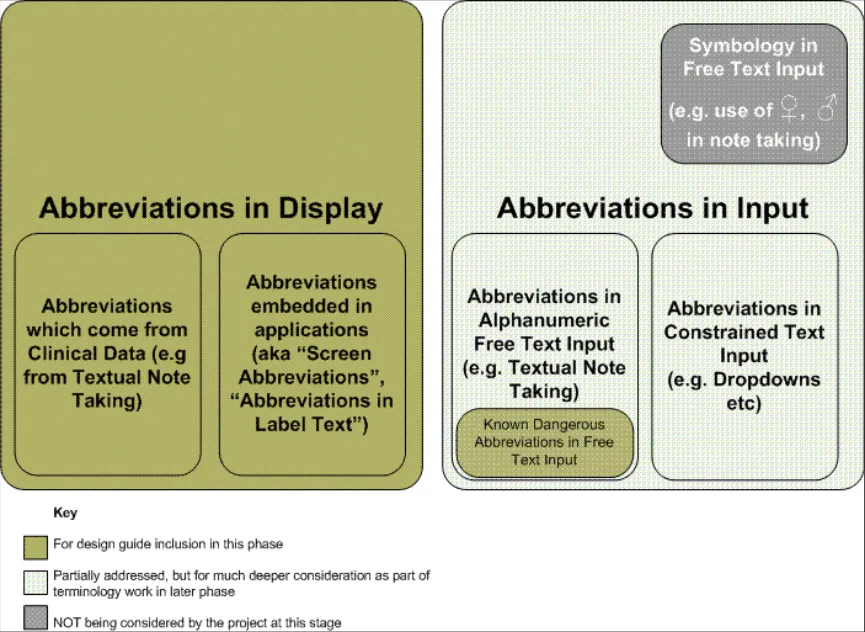
The following figure illustrates this documents scope of work and how it fits into the overall field of abbreviations and acronyms:
Figure 1: Taxonomy of abbreviations and acronyms, showing scope of work
As Figure 1 illustrates, it is not possible at this stage to make specific fully-validated recommendations around many areas of input abbreviation. However, this document presents guidance for display abbreviation and a specific subset of input abbreviation relating to known dangerous abbreviations (KDAs).
Future releases of this document will cover input abbreviation handling, including free text input (FTI). A separate appendix presents a suggested design approach for handling FTI containing abbreviations and acronyms. This design draws on current thinking within safety critical systems.
Note
This approach requires substantial further research for full validation and is therefore not presented as guidance.
Page 3
Copyright ©2013 Health and Social Care Information Centre
 HSCIC Controlled Document
HSCIC Controlled Document
3 GUIDELINES ON ABBREVIATION AND ACRONYM USAGE
This section presents each of the key guidelines on abbreviation and acronym usage that result from current research. The key guidelines will:
-
Require the user to resolve all known dangerous abbreviations and acronyms
-
Avoid or explain abbreviations and acronyms
-
Present abbreviations and acronyms consistently.
3.1 Require the User to Resolve all Known Dangerous Abbreviations and Acronyms
When accepting free text input which includes abbreviations, applications should require the user to resolve all known dangerous abbreviations and acronyms.
3.1.1 Recommendations
Applications which provide free text input, for example for note taking, should:
- Alert the user authoring the text to the presence of known forbidden/dangerous
abbreviations and acronyms (see below for a definition of these) whenever the author moves from one input field to another.
- Present potential expansions for selection where possible, but not provide a default
expansion.
- Prevent the storage of any such items under all circumstances.
The definition of a forbidden/known dangerous abbreviation or acronym is “one which is categorised as such by an appropriate authority”. This might arise for several equally valid reasons:
-
Confusion with another acronym or abbreviation, with potential patient safety consequences
-
Relation to drugs, for example, drug names, dose amounts, dose frequencies and so on
-
Misinterpretation in some other way which might affect patient safety, or be unsafe for some
other reason
- It has caused a dangerous incident in the past.
The process of collating and validating the list of forbidden/dangerous acronyms will be an ongoing one and this guideline does not prescribe how it should be achieved or by what authority, although initial sources for the list are suggested (see the “Rationale for Recommendation” section below) based on primary and secondary research.
3.1.2 Accessibility
The detailed accessibility considerations for this guidance will depend on the precise design adopted to adhere to the guidance. However several issues will have to be addressed by any design:
- The interaction design for alerting the user to the presence of dangerous unexpanded
items, and allowing users to select the next dangerous unexpanded item, will have to be usable by screen reader users and those who prefer or require keyboard or other input devices rather than mouse input.
- The interaction design for distinguishing between non-dangerous and dangerous
unexpanded items will need to use more than colour to do so.
Page 4
Copyright ©2013 Health and Social Care Information Centre
HSCIC Controlled Document
3.1.3 Justification
Some forms of abbreviation and acronym are known to be dangerous from specific experiences. The US National Patient Safety Guidelines (NPSG) Goal 2b (1) mandates a list of forbidden/dangerous abbreviations which is enforced by audit of patient notes for all accredited institutions. This list is deliberately constrained to those items which have caused incidents in the past, and it is therefore beneficial to avoid using the items on it. It is also clearly evidence-based. The list is reproduced in APPENDIX A
It is well recognised that abbreviation of drug names, dosage amounts, dose frequency etc is dangerous. The US Institute for Safe Medication Practices (ISMP) maintains a list of known dangerous drug-related abbreviations and acronyms which the NPSG references. This list is reproduced in APPENDIX B.
In addition to these secondary sources, as part of the NHS CUI project, ca 4500 abbreviations and acronyms in use across the NHS have been collated and categorised. The data has been analysed for collisions between acronym and abbreviation definitions, in particular looking for collisions between clinical terms or other items which might cause dangerous misinterpretation. This has revealed around 30 potentially dangerous acronyms which are also candidates for inclusion on a list of forbidden/dangerous abbreviations and acronyms. This list is reproduced in APPENDIX C.
3.1.4 Patient Safety
Observation of this guideline is critically important to patient safety. If applications do not resolve all known dangerous abbreviations and acronyms at input time, then clinicians may:
- Enter text into a clinical application which may be dangerously misleading or ambiguous to
other application users
- View information in clinical applications containing potentially dangerous abbreviations and
acronyms
- Receive no warning when reading medical text that potentially dangerous abbreviations and
acronyms are present, and may act on a mistaken impression of the intent of the author of the text – with possible negative consequences for patients.
This confusion could have unintended or hazardous results, for example:
-
Patients receiving the wrong drug or an incorrect dosage
-
Incorrect patient administration or clinical interaction due to mistaken abbreviations.
Appendices A,B and C provide more details of other possible dangerous conflicts.
3.2 Avoid or Explain Abbreviations and Acronyms
Applications should avoid abbreviation where possible. If it is not possible to avoid using an acronym, the user should have easy access to an explanation of the acronym’s meaning.
3.2.1 Recommendations
Applications which display labels (static text displayed by an application, for example, next to a form field to indicate what the field contains- also known as “Screen Text”) should:
-
Avoid using abbreviations and acronyms wherever possible - this is the preferred approach.
-
Use abbreviations and acronyms when screen space constraints would lead to horizontal
scrolling or clipping of the text if the fully expanded form were used instead.
- Use abbreviations and acronyms when clear evidence exists that they are universally used
or accepted in the target context for the application, and are more usable in their contracted forms.
Page 5
Copyright ©2013 Health and Social Care Information Centre
HSCIC Controlled Document
- Avoid using known dangerous abbreviations and acronyms regardless of screen or other
constraints.
- Provide a method of discovering the local meaning of the abbreviation or acronym where it
is not possible to avoid use, unless the user explicitly opts not to display this discovery method.
Methods for discovering the local meaning of an abbreviation or acronym must be:
-
Simple to use
-
Quick to use
-
Accessible to all users (for example, through a glossary link or other form of user
assistance).
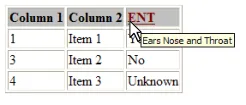
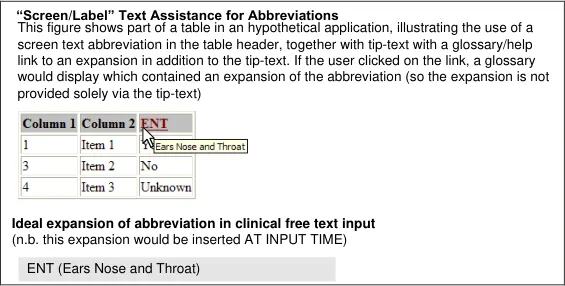
3.2.2 Examples
The figure below shows several views which conform to the recommendations in this document.
Note
These views do not dictate a particular interaction but merely illustrate interactions which comply with the guidance.
Figure 2: Example Views illustrating Explanation of an Abbreviation
3.2.3 Accessibility
When providing assistance for expanding abbreviations, applications must expose the explanation of the abbreviation in a manner which is accessible to all users, including users of assistive technologies such as screen readers, users with limited manual dexterity and users with low vision.
In particular it is not safe for an application to rely on tool-tips alone as a means of providing expansions, because:
-
They cannot be used by non-mouse users
-
It may be difficult for those with low vision to read them since they do not resize with other
text in a web context
- Those with limited manual dexterity may find them difficult to access.
3.2.4 Justification
Complexity is a well known source of human error (see for example the reference to Thomas Nolan ( 3 ) ). In this case, it is clear that more mental effort is required for a user to expand an abbreviation or acronym than it would be required to read the fully expanded form directly. This added effort (increased cognitive load) increases the risk of the user making a mistake in using the data presented, and makes mistakes in other activities more likely. In addition, in common with
Page 6
Copyright ©2013 Health and Social Care Information Centre
 HSCIC Controlled Document
HSCIC Controlled Document
other usages, the potential for ambiguity exists whenever abbreviations and acronyms are employed.
However it will not always be possible to display a fully expanded version of a long label (for example, where screen space is at a premium or the alternative to abbreviation would be horizontal scrolling), so in these cases it is important to mitigate the ambiguity risk by providing the user with access to the correct expansion.
Using the expanded form of an abbreviation will not be the best approach when it is clear (for example, from the user’s context) that they do not benefit from the expansion. This can arise because they are very familiar with the abbreviated form and will read and recognise it more quickly than the expanded form. In these cases the user’s cognitive load and reading time may be increased rather than decreased by the presence of the expanded form. When this argument is used for including an abbreviation, it must be substantiated by clear evidence of the common usage and understanding of the abbreviation in question however.
3.2.5 Patient Safety
These guidelines are important because if they are not observed:
- Abbreviations and acronyms will be used unnecessarily, adding to the increased cognitive
load of users and making user errors more likely.
- When abbreviations and acronyms do need to be used, users will not be able to determine
the correct meaning of acronyms they find and may make incorrect assumptions about the meaning, leading to error.
3.3 Present Abbreviations and Acronyms Consistently
When displaying abbreviations and acronyms, applications should always present them consistently with respect to capitalization and punctuation.
3.3.1 Proposed Guidance
Applications which display acronyms or abbreviations should:
- Present all acronyms (phrases reduced to their initial letters only) in UPPERCASE with no
punctuation marks and no interior spaces, for example, ENT for Ears, Nose and Throat rather than E N T, ent or E.N.T.
- Present all abbreviations (phrases truncated to two or more letters of their component
words) with every word or abbreviated word capitalized, and all truncated words punctuated with a full stop and no interior spaces, for example, Tib.Ant. for Tibialis Anterior, rather than TibAnt, Tib. Ant., tibant or tib ant)
Page 7
Copyright ©2013 Health and Social Care Information Centre
HSCIC Controlled Document
4 ACCESSIBILITY
The punctuation convention proposed may cause some difficulty for screen reader users. Some screen readers read out the acronym as a phrase, rather than pronouncing its individual letters (for example, ENT may be pronounced as the word “ent” rather than as the separate letters E N T). This suggests that a punctuated form with separators (E.N.T.) would be more accessible to screen reader users. However, any such suggestion needs to be weighed against the consequence of introducing an unfamiliar form to non-reader users, and the fact that screen reader users may already be very familiar with the “word forms” of common acronyms because of current usage. User research should be performed to optimise the recommendation.
In some circumstances it will be possible to mark the acronym as being an acronym in a machinereadable form, allowing assistive technologies such as readers to take appropriate action, such as reading out the letters individually. In HTML web applications this is achieved using the ACRONYM or ABBR tags. However some current readers do not interpret these representations correctly, so it is important that any recommendation stands independent of them.
4.1.1 Justification
Consistent presentation always enhances readability, and reduces the complexity of user interactions with the application interface. Reduced complexity enhances the safety of user interactions with the application.
Consistent presentation is particularly important with abbreviations since the user has to cope with the process of expanding the abbreviation. Inconsistent presentation adds another mental hurdle and contributes to usage errors, slowing the processing of patient information.
For these reasons, a set of guidelines for presentation which is consistent with common usage in glossaries found in the NHS and elsewhere is being proposed. This common usage is derived from observations made during the survey of ca 4500 abbreviations and acronyms in use across the NHS performed as part of the NHS CUI project. The rationale for following common usage is that the forms of presentation used should be familiar to clinicians and therefore yield the best chance of minimising the complexity of the display to the user.
4.1.2 Patient Safety
These guidelines are important because if they are not observed:
- Abbreviations and acronyms will be presented in many differing forms from application to
application, adding to the cognitive load of users and making user errors more likely.
- Users will be more likely to misinterpret the acronyms or abbreviations if they are not
presented consistently.
Page 8
Copyright ©2013 Health and Social Care Information Centre
HSCIC Controlled Document
5 TAXONOMY OF ABBREVIATION AND ACRONYM USAGE
It is helpful in thinking about abbreviation and acronym usage to organize their potential uses into categories for consideration, each of which has its own set of requirements and issues. The following table presents a simple taxonomy for observations in relation to abbreviations and acronyms.
Input Free Text (for example, Note Taking)
Input Constrained Text (for example, drop down boxes, radio button lists etc)
Any text may be entered. Impeding the flow of text input to expand abbreviations will dramatically reduce usability.
Rules can be similar to display of label text. Capable of being much more inherently safe than free text input of the same data with respect to abbreviation risks.
Display Label text Often possible to avoid abbreviation altogether, and always possible to provide assistance to explain those abbreviations which are necessary.
Display User-input text Reduction of ambiguity hinges on good input validation to remove ambiguity and highlight the remaining ambiguous text.
Special Drug-related information (for example, units of measure, dosages etc)
Scenarios where this data type is frequently exchanged (for example prescribing) should be considered for special UI treatment to avoid some of the most common hazardous abbreviations. However this sort of data often finds its way into free text notes where constraints are more difficult to enforce.
Table 1: Simple taxonomy for observations in relation to abbreviations and acronyms
Copyright ©2013 Health and Social Care Information Centre
Page 9
HSCIC Controlled Document
6 RESEARCH AND PROTOTYPING
All guidance in this document is based on current research. However, in some cases this research is not sufficient to justify the recommendations completely.
The potential design approach that “Abbreviations and Acronyms in Free Text Input.doc” provides is based on general safety system design principles and requires further work to justify.
The following items of research and prototyping are proposed in order to strengthen the research base for the guidance. Some of the items can logically be undertaken by the Microsoft CUI project team, but others require specialist clinician involvement in their organisation, execution and analysis.
6.1 Proposed Primary Research
Both these items of primary research are likely to need specialist clinician involvement in their organisation, execution and analysis.
6.1.1 Review of Current Practice in Ambiguity Resolution
A key tenet of the proposal for free-text input is that systems will be made safer if readers of notes are provided with information which:
- As far as possible contain fully expanded renderings of all abbreviations and acronyms
used
-
Contains NO known dangerous abbreviations
-
Warns them about the presence of unexpanded abbreviations and acronyms where
expansion has not been possible.
In order to prove the value of these proposals, particularly the last one, data should be collected on how clinicians in different scenarios currently resolve ambiguity which is present in paper medical records and notes, for example during handovers. This will show whether a system which can help quick recognition of ambiguity would be as helpful as anticipated.
6.1.2 Review of Proposed Forbidden or Dangerous Abbreviations and Acronyms
The same research subject group used above could also be used to gather data on candidate dangerous/forbidden abbreviations to validate them.
An ongoing piece of work will be required to update the list based on any adverse events involving abbreviation.
6.2 Candidates for Prototyping and User Testing
These items can sensibly be undertaken by the Microsoft CUI Project Team.
6.2.1 Free Text Input Panel with Ambiguity Resolution
In order to test the basic usability and acceptability to end users of the ideas embodied in the Free Text Input recommendations, we should design and build a prototype of a free text entry panel with general text ambiguity resolution which meets the guidelines, and test it with sample user groups. This is a complex piece of work and will probably require development team involvement in addition to interaction design work.
Page 10
Copyright ©2013 Health and Social Care Information Centre
HSCIC Controlled Document
6.2.2 Text Display Panel with Ambiguity Indication
In parallel with the above, a companion display which mocks up approaches for displaying data, and contains known unexpanded abbreviations and acronyms, should be designed and user tested.
6.2.3 Candidate for Office Workstream Inclusion
Much text input in the NHS will take place in Microsoft Word documents for several years to come, so it is vital that as much as possible of the free-text input recommendations be augmented by an NHS-specific Office feature. This feature can be proposed for development to the Office Workstream thereby allowing patient safety benefits to be delivered early.
The proposed feature would:
-
Allow an author to be alerted to unexpanded abbreviations and acronyms
-
Provide (on demand) a set of potential expansions for insertion
-
Alert the author to the inclusion of any known dangerous/forbidden abbreviations.
The feature would be refined and incorporated into the Office Workstream’s schedule of activities and a plan for its development produced.
6.2.4 Ensuring Consistency of Approach with Medical Terminology Handling
For many systems, it will be necessary to arrive at an approach for handling the input of notes and their transformation into systematic medical terminology (for example, coding for SNOMED-CT) which solves the same problem of resolving ambiguous input into unambiguous output. Whatever approach is adopted for free text handling regarding abbreviations and acronyms, the approach taken for terminology coding must be the same for consistency.
Page 11
Copyright ©2013 Health and Social Care Information Centre
HSCIC Controlled Document
7 REFERENCES
-
US National Patient Safety Guidelines 2004,5, Goal 2B, http://www.jcaho.org/accredited%2Borganizations/05_npsg_guidelines_3.pdf
-
US Institute for Safe Medication Practices “Do Not Use” list,
http://www.ismp.org/msaarticles/specialissuetable.html
- System changes to improve patient safety, Thomas W Nolan, BMJ 2000;320:771-773 ( 18 March ) http://bmj.bmjjournals.com/cgi/content/full/320/7237/771
Note
At the time of writing this document, websites are referenced using active hyperlinks to the correct web page. Due to the dynamic nature of websites, in time these links may become invalid.
Page 12
Copyright ©2013 Health and Social Care Information Centre
HSCIC Controlled Document
APPENDIX A JOINT COMMISSION ON ACCREDITATION
OF HEALTHCARE ORGANIZATIONS (US)
The following information is from the Official “Do Not Use” List from the Joint Commission on Accreditation of Healthcare Organizations Web site, at http://www.jcaho.org/accredited+organizations/patient+safety/06_dnu_list.pdf
U (unit) Mistaken for “0” (zero), the
number “4” (four) or “cc”
Write “unit”
IU (International Unit) Mistaken for IV (intravenous) or the number 10 (ten) Write “International Unit”
Q.D., QD, q.d., qd (daily) Q.O.D., QOD, q.o.d, qod
(every other day)
Trailing zero (X.0 mg)*
Lack of leading zero (.X mg)
MS
MSO4 and MgSO4
Table 2: Excerpt from the Official “Do Not Use” list
Mistaken for each other
Period after the Q mistaken for “I” and the “O” mistaken for “I”
Write “daily”
Write “every other day”
Decimal point is missed Write X mg
Write 0.X mg
Can mean morphine sulfate or magnesium sulfate
Confused for one another
Write “morphine sulfate”
Write “magnesium sulfate”
Additional abbreviations, acronyms and symbols (for possible future inclusion in the Official “Do Not Use” List).
- (greater than)
< (less than)
Misinterpreted as the number “7” (seven) or the letter “L”
Confused for one another
Write “greater than”
Write “less than”
Write drug names in full
Use metric units
Write “at”
Write “ml” or “millilitres”
Write “mcg” or “micrograms”
Abbreviations for drug names Misinterpreted due to similar
abbreviations for
multiple drugs
Apothecary units Unfamiliar to many practitioners
Confused with metric units
@ Mistaken for the number
“2” (two)
cc Mistaken for U (units) when
poorly written
μg Mistaken for mg (milligrams)
resulting in one thousand-fold
overdose
Table 3: Additional abbreviations and acronyms for possible future inclusion in the Official “Do Not Use” list
Copyright ©2013 Health and Social Care Information Centre
Page 13
HSCIC Controlled Document
APPENDIX B INSTITUTE OF SAFE MEDICAL PRACTICE (US)
The following table of dangerous abbreviations or dose designations is from the Institute of Safe Medical Practice Web site, at http://www.ismp.org/msaarticles/specialissuetable.html.
Apothecary symbols dram minim
Misunderstood or misread (symbol for dram misread for “3” and minim misread as “mL”).
Use the metric system.
AU aurio uterque (each ear) Mistaken for OU (oculo uterque—each eye). Don’t use this abbreviation.
D/C discharge discontinue
Premature discontinuation of medications when D/C (intended to mean “discharge”) has been misinterpreted as “discontinued” when followed by a list of drugs.
Use “discharge” and “discontinue.”
Drug names Use the complete spelling for drug names.
ARAºA vidarabine cytarabineARAºC
AZT zidovudine (RETROVIR)
CPZ COMPAZINE (prochlorperazine)
DPT DEMEROLPHENERGANTHORAZINE
azathioprine
chlorpromazine
diphtheria-pertussis-tetanus (vaccine)
HCl hydrochloric acid potassium chloride (The “H” is misinterpreted as “K.”)
HCT hydrocortisone hydrochlorothiazide
HCTZ hydrochlorothiazide hydrocortisone (seen as HCT250 mg)
MgSO4 magnesium sulfate morphine sulfate
MSO4 morphine sulfate magnesium sulfate
MTX methotrexate mitoxantrone
TAC triamcinolone tetracaine, ADRENALIN,cocaine
ZnSO4 zinc sulfate morphine sulfate
Stemmed names
“Nitro” drip nitroglycerin infusion sodium nitroprusside infusion
“Norflox” norfloxacin NORFLEX
m g microgram Mistaken for “mg” when handwritten. Use “mcg.”
o.d. or OD once daily Misinterpreted as “right eye” (OD—oculus dexter) and administration of oral medications in the eye.
Use “daily.”
TIW or tiw three times a week. Mistaken as “three times a day.” Don’t use this abbreviation.
per os orally The “os” can be mistaken for “left eye.” Use “PO,” “by mouth,” or “orally.”
q.d. or QD every day Mistaken as q.i.d., especially if the period after the “q” Use “daily” or “every day.”
Page 14
Copyright ©2013 Health and Social Care Information Centre
HSCIC Controlled Document
qn nightly or at bedtime Misinterpreted as “qh” (every hour). Use “nightly.”
qhs nightly at bedtime Misread as every hour. Use “nightly.”
q6PM, etc. every evening at 6 PM Misread as every six hours. Use 6 PM “nightly.”
q.o.d. or QOD every other day Misinterpreted as “q.d.” (daily) or “q.i.d. (four times daily) if the “o” is poorly written.
sub q subcutaneous The “q” has been mistaken for “every” (for example, one heparin dose ordered “sub q 2 hours before surgery” misunderstood as every 2 hours before surgery).
Use “every other day.”
Use “subcut.” or write “subcutaneous.”
SC subcutaneous Mistaken for SL (sublingual). Use “subcut.” or write “subcutaneous.”
U or u unit Read as a zero (0) or a four (4), causing a 10-fold overdose or greater (4U seen as “40” or 4u seen as 44”).
“Unit” has no acceptable abbreviation. Use “unit.”
IU international unit Misread as IV (intravenous). Use “units.”
cc cubic centimetres Misread as “U” (units). Use “mL.”
x3d for three days Mistaken for “three doses.” Use “for three days.”
BT bedtime Mistaken as “BID” (twice daily). Use “hs.”
ss sliding scale (insulin) or ½ (apothecary)
- and < greater than and less than
/ (slash mark) separates two doses or indicates “per”
Mistaken for “55.” Spell out “sliding scale.” Use “one-half” or use “½.”
Mistakenly used opposite of intended. Use “greater than” or “less than.”
Misunderstood as the number 1 (“25 unit/10 units” read as “110” units.
Do not use a slash mark to separate doses. Use “per.”
Name letters and dose numbers run together (for example, Inderal40 mg)
Zero after decimal point (1.0)
No zero before decimal dose (.5 mg)
Inderal 40 mg Misread as Inderal 140 mg. Always use space between drug name, dose and unit of measure.
1 mg Misread as 10 mg if the decimal point is not seen. Do not use terminal zeros for doses expressed in whole numbers.
0.5 mg Misread as 5 mg. Always use zero before a decimal when the dose is less than a whole unit.
Table 4: Dangerous abbreviations or dose designations
Copyright ©2013 Health and Social Care Information Centre
Page 15
HSCIC Controlled Document
APPENDIX C POTENTIALLY DANGEROUS AMBIGUOUS ABBREVIATIONS AND ACRONYMS
The following potentially dangerous abbreviations and acronyms resulted from the NHS CUI glossary consolidation exercise:
AE Adverse Event www.ukmi.nhs.uk/research/common_abreviations.asp
AE Air entry Chartered Society of Physiotherapy
amp ampoule www.dmd.nhs.uk/documentation.asp
AMP Austin Moore Prosthesis
Chartered Society of Physiotherapy
BTL Bilateral tubal ligation Chartered Society of Physiotherapy
btl bottle www.dmd.nhs.uk/documentation.asp
CMV Controlled mandatory ventilation
Chartered Society of Physiotherapy
CMV Cytomegalovirus www.dmd.nhs.uk/documentation.asp
CNS Central nervous system
CNS Coagulase negative streptococci
www.show.scot.nhs.uk/sign/guidelines/fulltext/53/abbreviations.html
www.bwhct.nhs.uk/index/about-clinicalreport/about-clinicalreport-abbreviations.htm
www.show.scot.nhs.uk/sign/pdf/sign28.pdf Chartered Society of Physiotherapy
www.show.scot.nhs.uk/sign/guidelines/fulltext/45/abbreviations.html
CP Cerebral palsy Chartered Society of Physiotherapy
CP Chondromalacia patellae
www.kneeguru.co.uk/html/dictionary/abbreviations.html
CRC Colorectal cancer www.show.scot.nhs.uk/sign/guidelines/fulltext/67/abbreviations.html
CRC Concentrated red cells www.show.scot.nhs.uk/sign/guidelines/fulltext/54/abbreviations.html
CRM Circumferential resection margin
www.show.scot.nhs.uk/sign/guidelines/fulltext/67/abbreviations.html
crm cream www.dmd.nhs.uk/documentation.asp
CVS Cardio Vascular System
Chartered Society of Physiotherapy
CVS Chorionic Villus biopsy www.bwhct.nhs.uk/index/about-clinicalreport/about-clinicalreport-abbreviations.htm
ER Equilibrium Reaction Chartered Society of Physiotherapy
ER Oestrogen receptor www.show.scot.nhs.uk/sign/guidelines/fulltext/29/abbreviations.html
ES Electrical stimulation www.show.scot.nhs.uk/sign/guidelines/fulltext/64/abbreviations.html
ES Embryonic Stem www.bwhct.nhs.uk/index/about-clinicalreport/about-clinicalreport-abbreviations.htm
FET Forced expiration technique
FET Frozen Embryo Transfer
Chartered Society of Physiotherapy
www.bwhct.nhs.uk/index/about-clinicalreport/about-clinicalreport-abbreviations.htm
FH Familial www.show.scot.nhs.uk/sign/guidelines/fulltext/40/abbreviations.html
Copyright ©2013 Health and Social Care Information Centre
Page 16
HSCIC Controlled Document
FH Family History Chartered Society of Physiotherapy
IUD Inter uterine death Chartered Society of Physiotherapy
IUD Intra Uterine Device www.bwhct.nhs.uk/index/about-clinicalreport/about-clinicalreportabbreviations.htm,www.show.scot.nhs.uk/sign/guidelines/fulltext/42/abbreviations.html
LA Left Atrium Chartered Society of Physiotherapy
LA Local anaesthetic www.show.scot.nhs.uk/sign/guidelines/fulltext/53/abbreviations.html
LDH Lactate dehydrogenase
www.show.scot.nhs.uk/sign/pdf/sign28.pdf
LDH Low dose heparin www.show.scot.nhs.uk/sign/guidelines/fulltext/56/abbreviations.html
MR Medial reefing www.kneeguru.co.uk/html/dictionary/abbreviations.html
MR modified-release www.dmd.nhs.uk/documentation.asp
P Pain Chartered Society of Physiotherapy
P Plan treatment Chartered Society of Physiotherapy
P Pulse Chartered Society of Physiotherapy
PD Parkinsons Disease Chartered Society of Physiotherapy
PD Postural drainage Chartered Society of Physiotherapy
PE Phenytoin equivalent www.show.scot.nhs.uk/sign/guidelines/fulltext/70/abbreviations.html
PE Pulmonary embolism www.show.scot.nhs.uk/sign/guidelines/fulltext/56/abbreviations.html,
www.show.scot.nhs.uk/sign/guidelines/fulltext/36/abbreviations.html
PE Pulmonary Embolus Chartered Society of Physiotherapy
PEP Positive Expiratory Pressure
PEP Pulmonary Embolism Prevention
Chartered Society of Physiotherapy
www.show.scot.nhs.uk/sign/guidelines/fulltext/56/abbreviations.html
PF Patello-femoral www.kneeguru.co.uk/html/dictionary/abbreviations.html,
Chartered Society of Physiotherapy
PF Pelvic Floor Chartered Society of Physiotherapy
PF Plantarflexion Chartered Society of Physiotherapy
PFS Patello-femoral syndrome
www.kneeguru.co.uk/html/dictionary/abbreviations.html
pfs pre-filled syringe(s) www.dmd.nhs.uk/documentation.asp
PH Past History Chartered Society of Physiotherapy
pH percentage hydrogen Chartered Society of Physiotherapy
PID Pelvic inflammatory disease
PID Prolapsed intervertebral disc
www.show.scot.nhs.uk/sign/guidelines/fulltext/42/abbreviations.html,
Chartered Society of Physiotherapy
Chartered Society of Physiotherapy
PNF Passive neck flexion Chartered Society of Physiotherapy
Copyright ©2013 Health and Social Care Information Centre
Page 17
HSCIC Controlled Document
PNF Proprioceptive neuromuscular facilitation
Chartered Society of Physiotherapy
PTB Partial thickness burn Chartered Society of Physiotherapy
PTB Patella tendon bearing Chartered Society of Physiotherapy
PV Cisplatin, vinblastine www.show.scot.nhs.uk/sign/pdf/sign28.pdf
PV Per vagina Chartered Society of Physiotherapy
PV Plasma viscosity Chartered Society of Physiotherapy
PV Pulmonary Vein Chartered Society of Physiotherapy
RA Rheumatoid arthritis www.kneeguru.co.uk/html/dictionary/abbreviations.html,
www.show.scot.nhs.uk/sign/guidelines/fulltext/48/abbreviations.html,
Chartered Society of Physiotherapy
RA Right Atrium Chartered Society of Physiotherapy
RR Respiratory Rate Chartered Society of Physiotherapy
RR Righting Reaction Chartered Society of Physiotherapy
SB Sinus bradycardia Chartered Society of Physiotherapy
SB Spina Bifida Chartered Society of Physiotherapy
SCC Spinal Cord Compression
SCC Squamous cell carcinoma
Chartered Society of Physiotherapy
Chartered Society of Physiotherapy
ST Sinus tachycardia Chartered Society of Physiotherapy
ST Soft Tissue Chartered Society of Physiotherapy
st standing Chartered Society of Physiotherapy
TKA Through knee amputation
TKA Total knee arthroplasty
Chartered Society of Physiotherapy
www.show.scot.nhs.uk/sign/guidelines/fulltext/54/abbreviations.html
VL Vastus Lateralis Chartered Society of Physiotherapy
vl vial(s) www.dmd.nhs.uk/documentation.asp
Table 5: Potentially dangerous abbreviations and acronyms
Copyright ©2013 Health and Social Care Information Centre
Page 18
HSCIC Controlled Document
REVISION AND SIGNOFF SHEET
Change Record
31-May-2005 Mark A.WilsonThomas
0.0.0.1 Extracted from “Abbreviations and Acronyms in Quick Wins Phase” v.0.5 for inclusion in Design Guide
1-Jun-2005 Anthony Steven 0.0.0.2 Light rewriting and reformatting of tables etc. Not a full developmental edit.
1-Jun-2005 Mark A.WilsonThomas
0.0.0.3 Reviewed rewrite and made minor corrections, simplified and removed repetition in introduction
2-Jun-2005 Anthony Steven 0.0.0.4 Prepared for customer review at conclusion of Quick Wins phase.
9-Jun-2005 Mark A.WilsonThomas
0.0.0.5 Modified figure AAA2.gif
Included comments about context for abbreviation.
30-Jun-2005 Anthony Steven 0.0.1.0 Quick Wins Release
07-Mar-2006 L Boardman-Rule 0.0.1.1 CopyEdit
12-Jun-2006 P Robinson 0.0.1.2 Author comments.
14-Jun-2006 L Boardman-Rule 0.0.1.3 Copyedit complete on author comments.
14-Jun-2006 L Boardman-Rule 0.0.2.0 Document Cleansed.
14-Jun-2006 Vivienne Jones 1.0.0.0 Baselined ready for conversion into PDF.
Document Status has the following meaning:
- Drafts 0.0.0.X - Draft document reviewed by the Microsoft CUI project team and the
Authority designate for the appropriate Workstream. The document is liable to change.
- Working Baseline 0.0.X.0 - The document has reached the end of the review phase and
may only have minor changes. The document will be submitted to the Authority CUI project team for wider review by stakeholders, ensuring buy-in and to assist in communication.
- Baseline Candidate 0.X.0.0 - The document has reached the end of the review phase and
it is ready to be frozen on formal agreement between the Authority and the Company
- Baseline X.0.0.0 - The document has been formally agreed between the Authority and the
Company
Note that minor updates or corrections to a document may lead to multiple versions at a particular status.
Reviewers
Jarnail Chudge 0.0.0.1 Design Guide Workstream Lead 31-May-2005
Paul Robinson 0.0.0.1 Program Manager 31-May-2005
Page 19
Copyright ©2013 Health and Social Care Information Centre
HSCIC Controlled Document
Distribution
Mark Farrer NHS CFH Director of Infrastructure
Document Properties
Document Title NHS CUI Design Guide Workstream Abbreviations and Acronyms
Author Mark A. Wilson-Thomas
Restrictions RESTRICTED – COMMERCIAL; MICROSOFT COMMERCIAL; Access restricted to: NHS CUI Project Team, Microsoft NHS Account Team
Creation Date
Last Updated 23 June 2015
Copyright:
You may re-use this information (excluding logos) free of charge in any format or medium, under the terms of the Open Government Licence. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence or email psi@nationalarchives.gsi.gov.uk.
Page 20
Copyright ©2013 Health and Social Care Information Centre